
Phase 5: Retrieval
Appointments
The day is here!!! The final day of this cycle. The day we have all been waiting for. Today’s not just your typical monitoring appointment; it’s retrieval day, and I’m so very ready to get these eggs out. The retrieval procedure takes place about 36 hours after the trigger injection, which signalled the follicles to prepare to ovulate. During ovulation, a follicle ruptures and expels the egg from the follicular sac, after which the egg will travel through the fallopian tube toward the uterus. Egg retrieval is timed to catch the eggs shortly before they would start this journey, at a point when they are ready for fertilization but are still within their follicles and can easily be found.

Here’s what my retrieval looked like:
1. After I checked in, I was guided to a private waiting room with my companion (who is also my boyfriend). Unfortunately, not every clinic offers this level of privacy so you may find yourself waiting and recovering with others in a room that’s divided up into semi-private areas with sheets. We both undressed; I put on my hospital gown and my companion put on scrubs and a hairnet. Then we waited for the nurse to arrive.
2. The nurse weighed me, checked my vitals, ensured I was the correct patient and got me comfy with a heating pad as I waited for the doctor to be ready.
3. The nurse gave me pre-procedure meds (see photo).
4. As part of my pre-procedure meds, I took a pain killer. Then I took an anti-nausea medication, “as a precautionary measure,” I was told.
5. I was escorted into the surgery room where I got on the exam table and put my legs in the stirrups. I was hooked up to an IV and the pain medication fentanyl was added to my drip. I began to feel the effects almost immediately and I started to relax. I grabbed my boyfriend’s hand and reminded myself: “Okay, I can do this.”
6. The doctor joined my boyfriend, the nurse and I in the surgery room. The doctor asked if I was ready and announced that he would start by “cleaning the vagina.” He then injected a freezing agent into the wall of my vagina to help with pain management and inserted the speculum. I can’t remember the exact order of these steps, thanks to the fentanyl, but you get the idea.

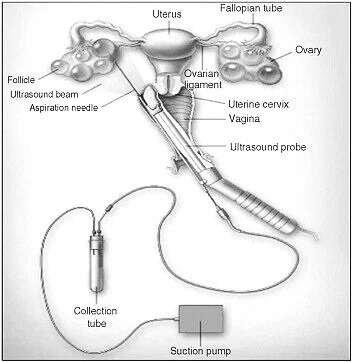
7. To retrieve the eggs, he placed a device into my vagina that kept the instruments steady and allowed him to push a needle through my vagina wall and into my ovary (see picture above). All these movements were guided by ultrasound technology connected to the needle. I felt a pretty significant “poke” in my right ovary as the needle broke through. Once the needle was inside my ovary, it was maneuvered to retrieve one egg after another. The fluid was drained through a small line into a test tube when the needle was inside a follicle. There was an embryologist in a lab that I could somewhat see through a small window-like door in the surgery room. She separated the fluid extracted from the follicles and counted the eggs retrieved as we went.
8. The nurse asked how I was doing and if I “need any more”—she was referring to fentanyl, and heck yes, please! The doctor okayed another two doses to keep me comfortable. I take as much pain medication as they are willing to give me to avoid unnecessary discomfort.
9. Next, the doctor announced he would move from my right ovary into the left one. “Alright, halfway over!” I told myself.
10. The nurse asked my boyfriend if he was okay. I think he was having a harder time than me! He was sweating, couldn’t look at the screen and was trying to distract me by talking about anything but what was happening. He’s a sweetheart, but I prefer to focus on my breath, so it’s almost as if I am not there. I took a deep breath and asked him to be quiet so that I could center myself.
11. OUCH! I felt a big poke in my left ovary. I didn’t feel the individual pokes into each sac, but the initial needle prick definitely got my attention. The doctor collected eggs and fluid from my left ovary just as he had done with the right one.
12. “We’re done!” the doc announced. Already? Whew! The nurse told me how brave I was, and the doctor told me these couples were so lucky—22 eggs were retrieved!
13. The nurse helped me up slowly, and I was sent back to my little private room to recover with my hydration IV bag.
14. I was given time to rest with a cookie and ginger ale. Thank god for that heating pad! It was the best thing in the world at that moment.
15. After about 40 minutes, a nurse checked on me and retook my vitals. I felt good enough to go, but the nurses weren’t sure yet. They left me to rest, and I updated my recipients. After about 90 minutes or so, we were sent home. The procedure generally lasts 20 to 30 minutes and is done on an outpatient basis, and you usually go home a few hours after the eggs are retrieved. This procedure is considered to be a minor surgery.
Medications:
I am all done with my egg donor medications!
Pre-procedure meds:
- Two acetaminophen (Tylenol®) for pain management
- Two celecoxib (CELEBREX®) to help with inflammation
- One lorazepam (Ativan) to help calm any pre-procedure anxiety
- One dimenhydrinate (GRAVOL™) to fend off nausea
- One gabapentin for pain management
Medication given by IV in the retrieval room:
- Fentanyl to manage pain during the procedure
- Midazolam for its sedative effect
- Cefazolin (Ancef) antibiotic to defend against infection
Side Effects
Risks from Anesthesia
Patients undergoing egg retrieval surgery generally rely on either intravenous anesthesia (where you are fully “asleep,” which is more prominent in the USA) or intravenous conscious sedation (where you are awake but heavily medicated, which is most commonly used in Canada) to handle their pain during the surgery. In general, anesthesia is safe, with deaths occurring only once every 200,000 to 300,000 cases. Because egg donors have so few of the factors that increase the risks of anesthesia (including being male, being older, being obese, having inpatient rather than outpatient surgery, and having surgery in an emergency setting), anesthesia should be even safer for egg donors than it is for surgical patients in general. The bottom line? The potential risks of anesthesia for egg retrieval are very low—outcomes feature rare mortality, rare major morbidity and rare minor morbidity.
Long-term Effects
Are there risks to our future health or fertility? We just don’t know. Most professionals say there are no risks to future fertility or other long-term risks; however, there is no database tracking donor health yet. If we aren’t researching the effects on donors long down the road, how can we say there’s no risk? I have personally talked to a number of donors and believe it would be naïve to think there are absolutely no ramifications from putting these artificial hormones into my body, but I truly don’t know what those may be/are. I have talked to women who have gone on to conceive just fine after donating 10 times, but I also know women who have had issues with their thyroid, night sweats and headaches that they associate with the change in their hormones. Everyone’s body is different, and it’s important to research potential side effects and weigh the pros and cons for yourself. If you’re feeling lost or overwhelmed, or you’d just like someone to discuss your decision with, don’t hesitate to contact me! I am more than happy to send you helpful resources and offer advice based on my personal egg-donation experience as well as my work as an egg donor coordinator, social worker and therapist.

Activity Restrictions
Avoid sex, amusement parks or any exercise more strenuous than walking in order to avoid ovarian torsion. Engaging in any of these activities while your ovaries are larger than usual could cause one to flip. Wait until you get your period. You can expect this anywhere from a few days to a week after your procedure. If you haven’t gotten your period after 7-10 days post-retrieval, reach out to your clinic.
Warning Signs
At this point, you’re just going to want to keep watching out for OHSS, which I have been talking about and providing tips for along the way.
Self-Care Tips
TAKE IT EASY, GIRL! You’re going to want to take in lots of electrolytes and salt, so drink sports beverages and broth in place of water. In order to help draw the fluid out of the ovaries and prevent accumulation in your abdomen, a high-sodium diet is recommended post-op. This also can help prevent OHSS. Though I wasn’t given a specific sodium amount, I wanted to consume 3,500 mg a day during the first five days post-retrieval. I set a “bare minimum” goal of 30+ grams a day if I fell short of 3,500 mg.
Focus on making a list and prepping at least three or four items ahead of time you may want to eat. I found chicken noodle soup to be high in sodium, tasty and light on the stomach! In, addition, have a heating bag handy and a friend or loved one nearby for support and any help around the house for those first 24 hours.
As much as you might want to, don’t have a bath for a week. Your parts just saw some major shit, and soaking in water allows the opportunity for that water to travel up your vagina. That water will likely be dirty, which leaves you at a risk for infection as you heal from the small punctures to your ovaries. Brief showers are your best bet until you’re fully healed.